
Quick Summary
Behavioral health claims fail at higher rates than other specialties because of documentation gaps, coding errors, authorization issues, and payer complexity. Improve your claims management by tightening documentation at the point of care, coding accurately, scrubbing claims before submission, submitting promptly, tracking claims through their lifecycle, working denials systematically, auditing your process regularly, and knowing when to outsource.
Why Behavioral Health Claims Are Different
Behavioral health claims get denied at higher rates than other medical specialties. Treatment spans weeks or months instead of single visits. Authorization requirements change mid-treatment. Documentation standards are more subjective. Many payers carve out behavioral health to separate administrators with their own rules.
A single denied claim costs $100-$250 to rework. Multiply that by dozens of denials per month and you’re looking at serious revenue leakage, plus the staff hours spent chasing payments instead of supporting patient care.
This Prosperity guide covers 8 strategies for improving your claims management process.
Why Listen to Us
Prosperity manages revenue cycle operations for behavioral health providers across substance use treatment, mental health practices, and multi-site residential programs.

Our clients maintain first-pass payment rates above 90% and denial rates under 5%. We process behavioral health claims daily and know what separates clean operations from chaotic ones.
How to Improve Claims Management
1. Get Documentation Right at the Point of Care
Most claim denials trace back to the clinical encounter, not the billing office. If documentation doesn’t support what you’re billing, the claim will fail.
Behavioral health documentation must establish medical necessity for every session. Payers want to see that the patient’s diagnosis supports the treatment provided, that measurable goals exist, and that progress (or clinical justification for continued care) is documented.
Vague notes like “patient had a good session” won’t survive a claim review.
The documentation must also match the billing code. If you’re billing a 60-minute psychotherapy session (90837), the note needs to reflect approximately 53+ minutes of psychotherapy. If you’re billing E/M services with a psychotherapy add-on, you may need separate documentation for each component.
Most behavioral health EHRs (Valant, Qualifacts/Credible, TherapyNotes, Kipu) include documentation templates designed for common service types. Use them. You should also configure your own templates to prompt clinicians for required elements.
2. Code Accurately
Coding errors are the most common trigger of preventable claim denials in behavioral health. The usual culprits are mismatched diagnosis and procedure codes, incorrect time-based code selection, missing or wrong modifiers, and outdated codes.
Behavioral health coding has specific nuances:
- Psychotherapy codes (90832, 90834, 90837) are time-based and must match documented session length
- Modifier 95 is required for telehealth with many payers
- When billing E/M with psychotherapy add-ons, the E/M code must be based on medical decision-making complexity, not total time spent
- Group therapy (90853) requires individual participant names for Medicare
Build a behavioral health-specific code reference your staff actually uses. Run quarterly training on coding updates since CPT changes annually. For complex claims, have a second set of eyes review before submission.
3. Scrub Claims Before Submission
Claim scrubbing catches errors before payers reject them.
You’re verifying that every required field is populated, codes are valid and properly paired, authorizations are in place and not expired, patient eligibility is confirmed, and provider credentials are current with the payer.
Most practice management systems include automated claim scrubbing that catches obvious errors like missing modifiers or invalid code combinations. Clearinghouses like Availity, Waystar, and Trizetto add another layer of validation before claims reach payers.
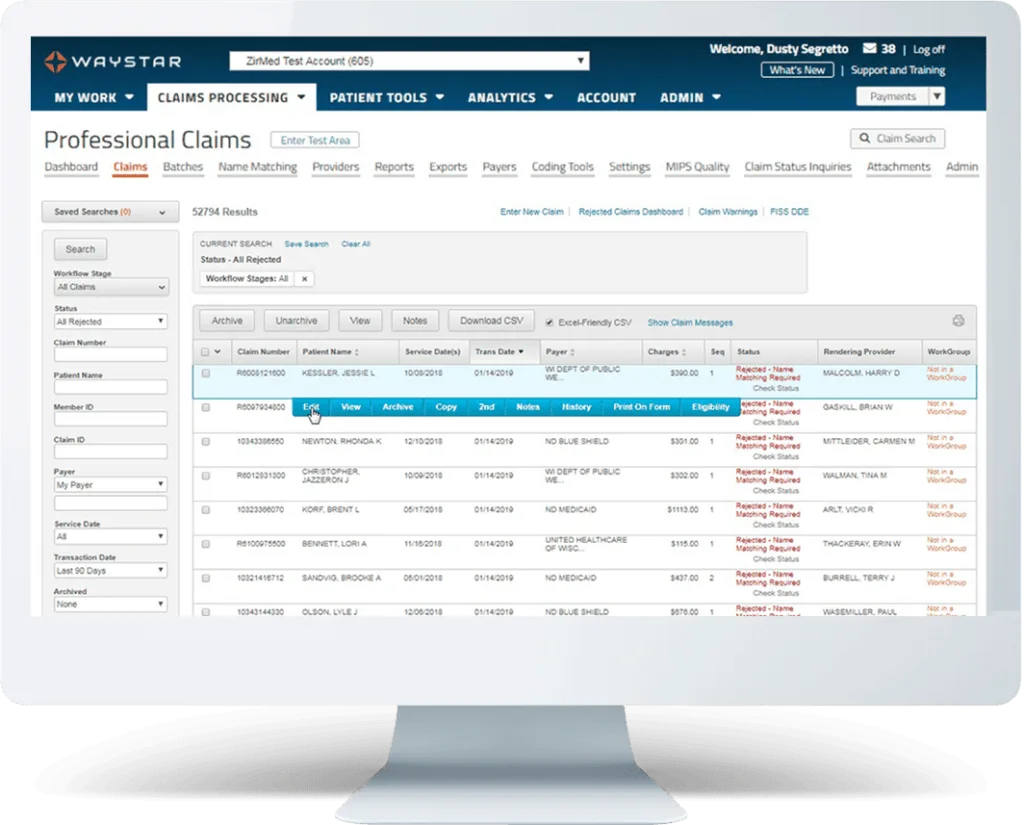
Source: Waystar
But behavioral health claims often need human review for nuances that software misses, particularly around authorization status and medical necessity documentation. Set a target of 95%+ of claims passing scrubbing on first attempt.
If you’re catching errors on more than 5%, you have upstream problems in documentation or coding.
4. Submit Claims Promptly
Timely filing deadlines vary by payer, but waiting to submit costs you money even when you’re within the deadline. Delayed submission means delayed payment, and it increases the chance that something gets entered incorrectly.
Submit claims daily, or at minimum every 48 hours. Same-day charge entry should be the goal for clinical services. Electronic submission through your clearinghouse is faster and more reliable than paper. Most commercial payers process clean electronic claims within 14-30 days, while paper claims can take 45+ days.
5. Track Claims Through the Lifecycle
Once claims are submitted, you need visibility into what happens. This means tracking claims from submission through adjudication, identifying claims pending too long, catching partial payments that should be investigated, and flagging patterns that indicate systematic problems.
Your practice management system or clearinghouse should provide a claims dashboard showing submission status, payer acknowledgment, and payment posting. Set up aging reports that flag claims at 30, 60, and 90 days. Review these weekly.
A claim sitting in limbo for 45 days is money you’re not collecting, and it may be approaching the point where you can’t easily fix whatever is wrong.
6. Work Denials Systematically
When claims deny, you need a structured process to resolve them. This starts with understanding the denial reason. Payers use Claim Adjustment Reason Codes (CARC) that tell you exactly why the claim was rejected or reduced.
Common behavioral health denial categories:
| Denial Type | Typical Causes | Resolution Approach |
| Authorization | Missing, expired, or invalid auth number | Verify auth was obtained; appeal with clinical documentation |
| Eligibility | Patient not covered on date of service | Confirm coverage was active; check for retroactive termination |
| Medical necessity | Documentation doesn’t support services | Appeal with strengthened clinical documentation |
| Coding | Invalid code, missing modifier, mismatch | Correct and resubmit; review for pattern of similar errors |
| Timely filing | Claim submitted past deadline | Limited options; document circumstances for appeal |
Work denials within 30 days. The longer you wait, the harder they are to resolve, and some appeal windows close entirely. Track denial resolution in your practice management system so nothing falls through the cracks.
7. Audit Your Process Quarterly
Most behavioral health practices work individual denials without ever addressing why those denials happened. The same errors repeat month after month.
Build a quarterly audit process:
- Pull your top 10 denial reasons by volume and dollar amount
- Map each denial category back to its originating workflow step (intake, documentation, coding, submission)
- Identify which denials were preventable vs. payer-driven
- Implement specific process changes for the top 2-3 preventable categories
If 15% of your denials are authorization-related, that’s an intake or utilization review problem, not a billing problem. If coding errors keep recurring, that’s a training gap. Treat denials as expensive feedback.
If you don’t have the bandwidth or expertise to audit your own process, Prosperity offers consulting engagements where we analyze your claims data, identify revenue leakage points, and recommend specific fixes. Sometimes an outside perspective catches patterns your team has stopped seeing.
8. Know When to Outsource
Running an effective claims management operation requires dedicated staff, specialized knowledge, ongoing training, and technology. For many behavioral health providers, this isn’t their core competency.
Outsourcing makes sense when your denial rate exceeds 5-10%, when claims sit in A/R for 45+ days on average, when your team lacks behavioral health-specific billing expertise, or when you’re growing faster than your billing operation can scale.
The key is finding a partner who understands behavioral health.
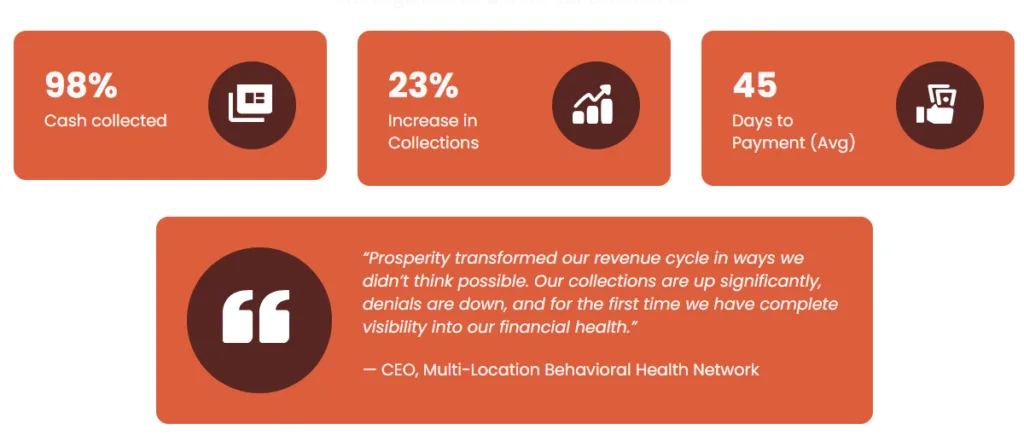
Prosperity provides full-service revenue cycle management for behavioral health providers. We handle claims from charge entry through payment posting, denial management, and appeals. Our clients see first-pass payment rates above 90%, denial rates under 5%, and days to payment under 45 on commercial claims.
Stop Leaving Money on the Table
Most behavioral health claim denials are preventable. They come from documentation gaps, coding errors, missed authorizations, and process breakdowns that repeat because nobody is tracking patterns.
Tighten your documentation. Code accurately. Scrub before you submit. Track what happens. Work denials fast. Audit regularly. And if your team can’t keep up, find a partner who specializes in behavioral health billing.If your claims process is costing you more than it should, talk to Prosperity about RCM services.


{kind=link}
{kind=link}